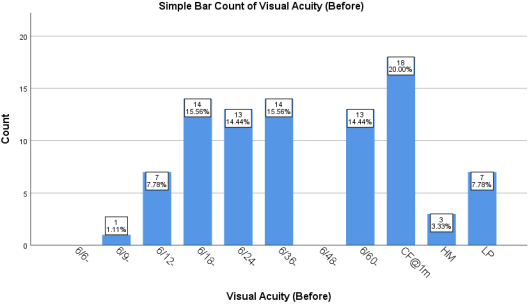
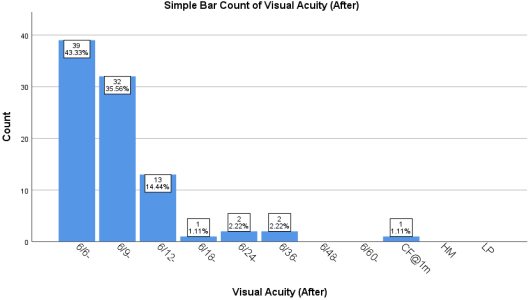
Background. The visual outcomes of phacoemulsification (Phaco) and manual small incision cataract surgery (MSICS) have been extensively studied, with research indicating that both methods are highly effective in restoring vision. Purpose. This study was aimed at comparing the visual acuity outcomes of the two surgical techniques. Methods. A total of 90 participants were scheduled for cataract surgery at Adetula Opticals & Eye Clinic, Oshodi-Isolo, Lagos State, Nigeria, from June to August 2023. The participants were divided into two groups of 45, a group was scheduled for Phaco (0.92 ± 0.65; 6/60-6/36) and SICS (1.32 ± 0.81; 3/60) logMAR. Visual acuities (VAs) were measured pre- and postoperatively. Results. The difference in mean VA pre-op of -0.40 (95% confidence interval (CI): -0.096, -0.71) between the two techniques was statistically significant (p = 0.000). There was no significant difference in the logMAR VAs between the techniques post-operatively (p = 0.06), although the visual outcome with the two methods showed the tendency of a better VA (0.11± 0.17 [6/9 - 6/6]) as opposed to that of the other two techniques (0.22 ± 0.32; [6/12 - 6/9]). Conclusion. Both techniques have been refined to a point where they provide comparable long-term visual outcomes, making the choice of method dependent on specific patient needs, surgeon expertise, and available resources.
| Published in | American Journal of Optics and Photonics (Volume 12, Issue 2) |
| DOI | 10.11648/j.ajop.20241202.12 |
| Page(s) | 30-36 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Phacoemulsification, Manual Small Incision Cataract Surgery, Logarithm of Minimum Angle of Resolution, Visual Acuity Outcomes, Comparison of Surgical Techniques
Visual acuity | Range | Mean VA ± SD | SE | 95% Confidence interval (Mean ± 1.96SE) |
|---|---|---|---|---|
VA Phaco Pre-op | 2.10 - 0.17 | 0.92 ± 0.65 | 0.097 | 1.12 - 0.73(n = 45) |
VA Phaco Post-op | 0.78 - 0.00 | 0.11 ± 0.17 | 0.025 | 0.16 - 0.061(n = 45) |
VA SICS Pre-op | 2.70 - 0.17 | 1.32 ± 0.81 | 0.12 | 1.57 - 1.08(n = 45) |
VA SICS Post-op | 2.10 - 0.00 | 0.22 ± 0.32 | 0.047 | 0.31 - 0.12(n = 45) |
Gender | Mean VA ± SD | SE | 95% Confidence interval |
|---|---|---|---|
Cum Surgery | (LogMAR Unit) | (Mean VA ± 1.96SE) | |
VA Pre-op | |||
Phaco & SICS | |||
Males (n = 42) | 1.03 ± 0.71 | 0.11 | 1.25 - 0.81 |
VA Pre-op | |||
Phaco & SICS | |||
Females (n = 48) | 1.20 ± 0.79 | 0.11 | 1.42 - 0.98 |
VA Post-op | |||
Phaco & SICS | |||
Males (n = 42) | 0.16 ± 0.18 | 0.03 | 0.22 - 0.10 |
VA Post-op | |||
Phaco & SICS | |||
Females (n = 48) | 0.17 ± 0.31 | 0.04 | 0.25 - 0.092 |
Phaco | Phacoemulsification |
MSICS | Manual Small Incision Cataract Surgery |
VAs | Visual Acuities |
ECCE | Extracapsular Cataract Extraction |
UCVA | Uncorrected Visual Acuity |
BCVA | Best Corrected Visual Acuity |
| [1] | Javitt JC, Wang F, West SK. Blindness due to Cataract: epidemiology and prevention. (1996). Annual Review of Public Health. 17: 159-177. |
| [2] | Fine, I. H., Packer, M., & Hoffman, R. S. (2001). Use of power modulations in phacoemulsification; choo-choo chop and flip phacoemulsification. Journal of Cataract and Refractive Surgery 27(2): 188-197. |
| [3] |
Riaz Y, de Silva SR, Evans JR. (2013). Phacoemulsification versus extracapsular cataract extraction for age-related cataracts. Cochrane Database System Review; CD004242.
https://doi.org/10.1002/14651858 CD004242.pub3. |
| [4] | Das N, Shams A, Kumar J, Khan B, Bhatti N. Visual outcomes of manual small incision cataract surgery versus phacoemulsification. Pakistan Journal of Ophthalmology 2021; 37(2): 123-128. |
| [5] | Ruit S, Tabin G, Chang D, et al. (2007). A prospective randomized clinical trial of phacoemulsification vs manual sutureless small-incision extracapsular cataract surgery in Nepal. American Journal of Ophthalmology 143(1): 32 - 38. |
| [6] | Gogate P, Deshpande M, Wormald R. (2003). Is manual small incision cataract surgery affordable in developing countries? Cost comparison with extracapsular cataract extraction. British Journal of Ophthalmology 87: 843-846. |
| [7] | Kumari R, Pradhan N, Gupta SK, Dubey G, Mohapatra A, Singh J, Ali J, Srivastava MR, Janardhanan R. (2021). Phacoemulsification versus Manual Small incision cataract surgery in Hard Nuclear Cataracts. Turkish Online Journal of Qualitative Injury 12(3): 700 -705 |
| [8] | Agrawal G, Patel D. (2024). Visual outcome and Complications of phacoemulsification and manual small incision cataract extraction for age-related Cataract. Indian Journal Clinical Experimental Ophthalmology 10(1): 170 -175. |
| [9] | Moussa G, Bassilious K, and Matthews N. (2021). A novel Excel sheet tool from Snellen fraction to logMAR including ‘Counting fingers’, ‘hand motion’, ‘light perception’, ‘no light perception’, and a focused review of literature of low visual acuity reference values. Acta Ophthalmologica e963 - e965. |
| [10] | Holladay JT (2004). Visual acuity measurements. Journal of Cataract and Refractive Surgery. 30: 287 - 290. |
| [11] | Holladay JT. (1997). Proper method for calculating average visual acuity. Journal of Refractive Surgery 13: 388-391. |
| [12] | Schultze-Bonsel K, Feltgen N, Burau H, Hansen L and Bach M. (2006). Visual acuities ’hand motion’, and ‘Counting fingers’ can be quantified with the Freiburg visual acuity test. Investigative Ophthalmology and Vision Science 47: 1236-1240. |
| [13] | Lange C, Feltgen N, Junker B, Schulze-Bonsel K, Bach M. (2009). Resolving the Clinical acuity Categories “hand motion”, and “Count fingers” using the Freiburg Visual Acuity Test (FrACT). Graefe’s Archive for Clinical and Experimental Ophthalmology 247(1): 137-142 |
| [14] | Day AC, Donachie PHJ, Sparrow JM, and Johnston RL. (2015). The Royal College of Ophthalmologists National Ophthalmology Database study of Cataract Surgery: Report 1, Visual Outcomes and Complications. Eye 29: 552-560. |
| [15] | Toyama T, Ueta T, Yoshitani M, Sakata R and Numaga J (2018). Visual acuity improvement after phacoemulsification cataract surgery in patients aged ≥90 years. BioMedical Central Ophthalmology 18(1): 280. |
| [16] | Waghmare RR, Shinde CA, Shirwadkar S. (2019). A Comparative study of Pre- and Post-operative Refractive Errors in Cataract Surgery-Phacoemulsification vs. Manual SICS in Tertiary Care Hospital. Journal of Evidence-Based Medical Health Care 6(51): 3212 - 3216. |
| [17] | Dervenis N, Praidou A, Dervenis P, Chiras D, and Littlea B. (2021). Visual acuity outcomes after Phacoemulsification in Eyes with Good visual acuity before cataract surgery. Medical Principle and Practice 30(3); 285-291. |
| [18] | Cox JT, Subburaman GB, Munoz B, Friedman DS, Ravindran RD. (2019). Visual Acuity Outcomes after Cataract Surgery-High-volume versus Low-volume Surgeons. Ophthalmology 126(11): 1480-1489. |
| [19] | Singh SK, Winter I and Surin L. (2009). Phacoemulsification versus Small Incision Surgery (SICS); which one is a better surgical option for immature cataracts? Nepal Journal of Ophthalmology 1(2): 95 - 100. |
| [20] | Ahmed I, Alvi RH, Maazallah A, Nizamuudin M. (2023). Comparison of visual outcomes between phacoemulsification and small incision cataract surgery. Journal of Liaquat National Hospital 1(2): 84-89. |
| [21] | Bhutto IA, Ali I, Memon MN, Bukhari AS, Indhar I, Memon NA. (2021). Comparison of visual outcome in senile cataract after phacoemulsification and manual small incision cataract surgery. International Journal of Endorsing Health Science Research 9(1): 143-148. |
| [22] | Surya PAAS and Sunariasih NN. (2021). Comparison of Visual acuity between post-Small Incision Cataract Surgery and Phacoemulsification in Sanjiwani Hospital. European Journal of Medical and Health Sciences 3(6): 101-104. |
| [23] | Norregaard JC, Hindsberger C, Alonso J, Bellan L, Bernth-Petersen P, Black C, Dunn E, Andersen TF, Espallargues E, Anderson GP. (1998). Visual outcomes of Cataract Surgery in the United States, Canada, Denmark, and Spain. Archive of Ophthalmology 116(8): 1095 - 1100. |
| [24] | Rono JK and Nirghin U. (2023). Visual outcomes after small incision cataract surgery of patients in Kenyan Hospital Contributors. African Health Sciences 23(2): 469 - 477. |
| [25] | Lundqvist B, Mönestam E and Jonsson AC. (2008). Gender-related differences in Cataract Surgery outcome: a 5-year follow-up. Acta Ophthalmologica Scandinavica. 86(5); 543-548. |
| [26] | Khan AM, Waldner DM, Luong M, Sanders E, Crichton ACS and Ford BA. (2022). Stabilization of refractive error and associated factors following small incision phacoemulsification cataract surgery. BioMedical Central Ophthalmology 13(1): 1-10. |
| [27] | Kumari V, Ali J, Janardhanan R, Dubey G, Saeed A, Kumari V, Ali J, Janardhanan R. (2020). A Comparative study to evaluate visual outcome in postoperative patients of small incision cataract surgery and phacoemulsification. Elementary Education Online 19(4): 3570 - 3576. |
APA Style
Iyamu, E., Okechukwu, C. I. (2024). Comparison of Visual Acuity Outcomes of Phacoemulsification and Small Incision Cataract Surgery. American Journal of Optics and Photonics, 12(2), 30-36. https://doi.org/10.11648/j.ajop.20241202.12
ACS Style
Iyamu, E.; Okechukwu, C. I. Comparison of Visual Acuity Outcomes of Phacoemulsification and Small Incision Cataract Surgery. Am. J. Opt. Photonics 2024, 12(2), 30-36. doi: 10.11648/j.ajop.20241202.12
@article{10.11648/j.ajop.20241202.12,
author = {Eghosasere Iyamu and Clinton Ifeanyi Okechukwu},
title = {Comparison of Visual Acuity Outcomes of Phacoemulsification and Small Incision Cataract Surgery
},
journal = {American Journal of Optics and Photonics},
volume = {12},
number = {2},
pages = {30-36},
doi = {10.11648/j.ajop.20241202.12},
url = {https://doi.org/10.11648/j.ajop.20241202.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajop.20241202.12},
abstract = {Background. The visual outcomes of phacoemulsification (Phaco) and manual small incision cataract surgery (MSICS) have been extensively studied, with research indicating that both methods are highly effective in restoring vision. Purpose. This study was aimed at comparing the visual acuity outcomes of the two surgical techniques. Methods. A total of 90 participants were scheduled for cataract surgery at Adetula Opticals & Eye Clinic, Oshodi-Isolo, Lagos State, Nigeria, from June to August 2023. The participants were divided into two groups of 45, a group was scheduled for Phaco (0.92 ± 0.65; 6/60-6/36) and SICS (1.32 ± 0.81; 3/60) logMAR. Visual acuities (VAs) were measured pre- and postoperatively. Results. The difference in mean VA pre-op of -0.40 (95% confidence interval (CI): -0.096, -0.71) between the two techniques was statistically significant (p = 0.000). There was no significant difference in the logMAR VAs between the techniques post-operatively (p = 0.06), although the visual outcome with the two methods showed the tendency of a better VA (0.11± 0.17 [6/9 - 6/6]) as opposed to that of the other two techniques (0.22 ± 0.32; [6/12 - 6/9]). Conclusion. Both techniques have been refined to a point where they provide comparable long-term visual outcomes, making the choice of method dependent on specific patient needs, surgeon expertise, and available resources.
},
year = {2024}
}
TY - JOUR T1 - Comparison of Visual Acuity Outcomes of Phacoemulsification and Small Incision Cataract Surgery AU - Eghosasere Iyamu AU - Clinton Ifeanyi Okechukwu Y1 - 2024/10/10 PY - 2024 N1 - https://doi.org/10.11648/j.ajop.20241202.12 DO - 10.11648/j.ajop.20241202.12 T2 - American Journal of Optics and Photonics JF - American Journal of Optics and Photonics JO - American Journal of Optics and Photonics SP - 30 EP - 36 PB - Science Publishing Group SN - 2330-8494 UR - https://doi.org/10.11648/j.ajop.20241202.12 AB - Background. The visual outcomes of phacoemulsification (Phaco) and manual small incision cataract surgery (MSICS) have been extensively studied, with research indicating that both methods are highly effective in restoring vision. Purpose. This study was aimed at comparing the visual acuity outcomes of the two surgical techniques. Methods. A total of 90 participants were scheduled for cataract surgery at Adetula Opticals & Eye Clinic, Oshodi-Isolo, Lagos State, Nigeria, from June to August 2023. The participants were divided into two groups of 45, a group was scheduled for Phaco (0.92 ± 0.65; 6/60-6/36) and SICS (1.32 ± 0.81; 3/60) logMAR. Visual acuities (VAs) were measured pre- and postoperatively. Results. The difference in mean VA pre-op of -0.40 (95% confidence interval (CI): -0.096, -0.71) between the two techniques was statistically significant (p = 0.000). There was no significant difference in the logMAR VAs between the techniques post-operatively (p = 0.06), although the visual outcome with the two methods showed the tendency of a better VA (0.11± 0.17 [6/9 - 6/6]) as opposed to that of the other two techniques (0.22 ± 0.32; [6/12 - 6/9]). Conclusion. Both techniques have been refined to a point where they provide comparable long-term visual outcomes, making the choice of method dependent on specific patient needs, surgeon expertise, and available resources. VL - 12 IS - 2 ER -
Department of Optometry, Faculty of Life Sciences, University of Benin, Benin, Nigeria
Department of Optometry, Faculty of Life Sciences, University of Benin, Benin, Nigeria